Body Composition and its Surprising Affect on Scoliosis
Introduction
Scoliosis is defined as the “three-dimensional deformity of the spine” with a curvature of the spine in the “coronal plane of more than 10 degrees”. To an amateur, this curvature can be simply described as the sideways warping of the spine. Adolescent idiopathic scoliosis (AIS) is the most common type of spinal deformity and is the type of scoliosis that will be investigated in this study. This is prevalent in people aged between 10 and 18 years old and has no known definitive cause. However, there are multiple factors that have been widely theorised to have a contributing effect on scoliosis. The most accepted of the factors I will include are genetic-hormonal causes, biomechanical causes, and genetic abnormalities.
Since there is no definitive cause, all of these factors have not been conclusively proven, which still leaves much research to be done on the strength and effects of other theories as well as more criticisms and review of the current theories to further determine their reliability and merit so that a final cause is found. This is primarily the reason that I have chosen this topic. I believe that the factor of body composition is not as widely investigated as some other factors (e.g., neuromuscular), and it is beneficial to review the rest of the causes to determine how strong of a factor it is compared to the other factors, as well as how they affect scoliosis.
Body composition
The first possible cause to be reviewed will be body composition, which is the factor the experiment conducted has investigated. In a review of studies done to examine the effects of BMI on scoliosis, there was a majority of studies which generally found a relationship between low BMI and scoliosis, which is the same trend that was found from our experiment. However, many other trends were found as well. A Korean study mentioned in this review found that whilst low BMI was significantly associated with the incidence of scoliosis, a higher BMI was actually “protective against the development” of idiopathic scoliosis in adolescents. This is because they found that the angle of scoliosis that they found in the severely underweight group of participants was significantly higher than that of those in the normal weight group. This is further supported by another study that compared Cobb angle to BMI and found that patients with AIS had a significantly lower BMI compared to those who did not have scoliosis. This same study found that there was also a positive relationship between significantly low body weight and those with scoliosis. This is different from the Korean experiment previously mentioned, the low weight alone was the factor for scoliosis, not the relative underweight body type therefore the lower BMI which correlated with our results.

This study therefore goes against the positive relationship found between solely weight and scoliosis from our results. In this same source, they found that lower muscle mass and higher fat mass could be related to the progression of scoliosis. If the trend found in this source and the results of a positive trend of muscle mass and negative trend of body fat percentage in my results are true, that leads us to believe that the effects of muscle mass and fat on scoliosis differs between genders. Another investigation on the effects of body composition values on scoliosis across a period of 5 years by M. Clark in the same review did show a negative correlation between body mass and scoliosis, yet also found an association between lean and fat mass. They found that an increase in lean mass showed a 20% reduction in the risk of scoliosis and an increase in fat mass reduced the risk of scoliosis by 13%. The idea of an increase in fat mass primarily (as well as lean mass) would support the claim from the Korean study that a higher BMI would protect against the development of scoliosis. The authors believed that the link of fat and lean mass to risk of scoliosis could be explained by traction or other mechanical mechanisms.
Genetic factors
The next factor that will be reviewed is the role of genetic factors on adolescent idiopathic scoliosis. Whilst it has always been known that genetic factors have been involved in the development of scoliosis, a study has shown that it is the underlying cause of it. A study has found that there are 16 genes to be reported and associated with scoliosis, such as FOXA2, EPHA4, and SOX9. Studies have also shown that the role of similar genes to these have been targeting bone metabolism and body growth, which could also affect body composition at the same time, hence linking the results of our experiment. Another gene (LBX1) is also a very influential gene that could lead to spinal curvature therefore a relationship to a development of adolescent idiopathic scoliosis. Whilst there needs to be a lot more research done into genetic factors, it is a very promising area as demonstrated in the study.

Environmental factors
Another study suggests that scoliosis is caused by environmental stress and factors. This supposedly causes developmental instability in the growth of the spine. The environmental factors could cover hormones, nutritional factors, drugs, toxins, and physical activity. Scoliosis has also been seen to occur in children due to psychological distress, or physical trauma, as well as treatments like chemotherapy and surgery. A favourite in the environmental factors is the idea that nutritional deficiency can affect scoliosis. An experiment involving over 70 children with skeletal abnormality has shown that all the children have low vitamin D, with most having low calcium intake. This leads us to believe that environmental factors involving nutrition are very influential to scoliosis as there is a very strong relationship between the two.
Biomechanics
Biomechanics are also viewed to be a possible cause of scoliosis as presented in an etiopathogenesis on scoliosis. This is because in scoliosis, there is “a difference between the growth of the anterior vertebral body and the growth of the posterior elements”. This abnormal growth between different positions of the spine results in lordosis which is the inward curvature of the spine in the lumbar and cervical regions of the spine. This is slightly different from scoliosis which is the sideways curvature of the spine. The reduced growth of the hindquarters leads to the vertebrae in the centre to stop growing in height which forces twisting of the spine to create space leading to rotational lordosis. It has been proven in multiple studies that lordosis is nearly always present in scoliosis therefore his could be a very promising factor.
Neuromuscular factors
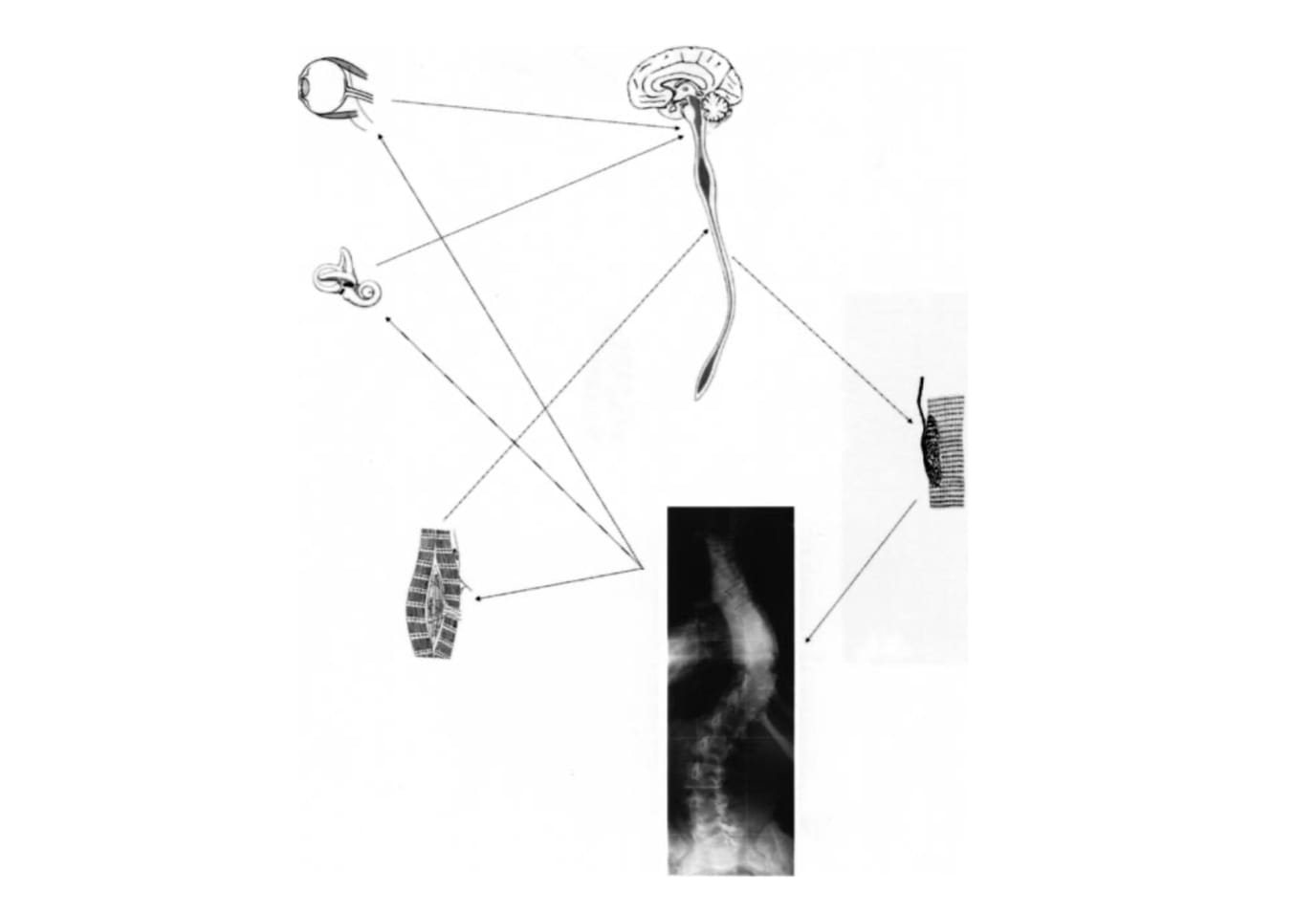
A European study suggests that defective postural equilibrium as a result of neuromuscular factors is a possible contributing factor in the development of scoliosis. This study suggests that “defects in visual and vestibular input” could be a contributing factor in the development of scoliosis. This effectively theorises that our ability to balance our body and our body awareness through our vestibular system (located in the inner ear) and vision can influence scoliosis. This is because the brain uses sensory information from the body to control posture as well as movement, and that postural instability could arise from this. Proprioception is another possible contributor as the body is able to sense where it is without the need for visual input through signals from the sensors in our muscles and joints. Therefore, this study proposes that a defective vestibular or proprioceptive system as well as incorrect visual input could lead to postural instability therefore the warped and incorrectly controlled growth of the spine leading to scoliosis. On top of this, the study references many experiments which have shown that the muscles on convex side of the spine are more active in scoliosis, which can also lead to an increased load and asymmetrical muscle growth, which also provides a convincing explanation for the gradual progression of idiopathic scoliosis with asymmetrical muscle growth.
The asymmetrical muscle growth can be linked with the results from our experiment which supports the positive relationship between muscle mass and scoliosis, if the perspective is that the higher asymmetrical muscle mass leads to a higher asymmetrical curve progression, yet this is just a theory.
Conclusion
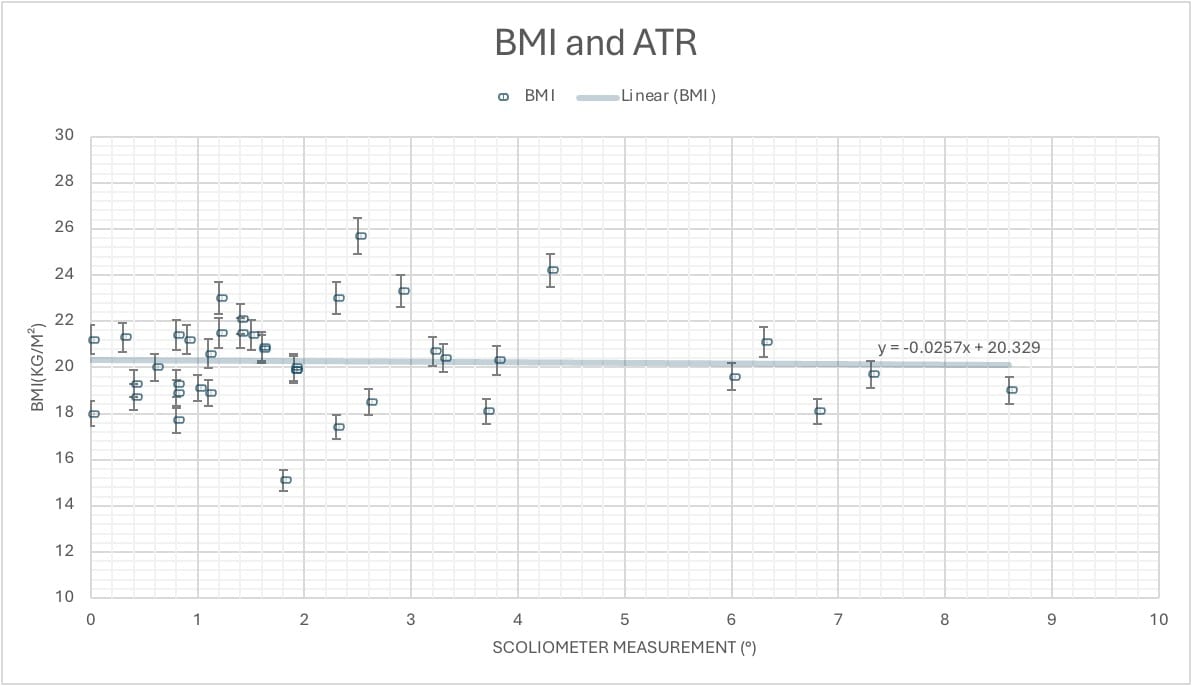
In conclusion, the hypothesis which stated that there will be a negative trend with scoliosis and BMI is true. However, this trend is further enhanced by the comparison of body fat percentage against scoliosis instead of BMI. This is due to the fact that as explained before, body fat percentage is a closer measurement to the real value of fat composition as opposed to BMI which does not consider the different body types. This is shown by the strong gradient of -0.1082 for body fat percentage and scoliosis compared to -0.0257 for BMI and scoliosis. Due to the support of the sources such as clinical reviews, articles, and experiments which all say there is much evidence to support this negative trend which I have also found, I believe that this is an area with a lot of promise and potential in being a large influencer of scoliosis. Overall, I conclude that scoliosis is still due to a combination of all the factors (excluding the minor theories), which include body composition, genetic factors, environmental factors, biomechanics, and neuromuscular factors. However, I believe that the environmental factors are extremely important and influential due to the very strong relationship between low intakes of vitamin D and calcium compared to scoliosis. With more research into this theory, I believe that it could be found to be one of the main influencers of scoliosis.